
America’s race problems reflect similar problems around the world.
According to AIDS.gov: “By race, blacks/African Americans face the most severe burden of HIV.”
According to the U.S. Department of Health & Human Services:
HIV/AIDS has had a devastating impact on minorities in the United States. Racial and ethnic minorities accounted for 70 percent of the newly diagnosed cases of HIV infection in 2011. In 2011, 82 percent of children born with HIV infection belong to minority groups.
In the African American community, HIV infections has become an epidemic. African Americans accounted for 44% of all HIV infections cases diagnosed in 2011. African American men are 7 times more likely to die of AIDS than non-Hispanic White men. African American women are particularly struck by this disease, and are 15 times more likely to die from HIV, as compared to non-Hispanic White women. AIDS is the fourth leading cause of death in African American women aged 35-44 and the fourth leading cause of death in African American men, aged 45-54, in 2010.
HIV/AIDS is spreading at a rapid rate in the Hispanic community. Hispanics accounted for 20 percent of AIDS cases in 2011, despite making up only 17 percent of the U.S. population. Hispanics are twice as likely to be diagnosed with AIDS than Whites. Hispanic males were also twice as likely to die of AIDS than their non-Hispanic White counterparts, and Hispanic women were 2.2 times more likely to die from AIDS.
Though the numbers are small, American Indians are also impacted disproportionately by HIV/AIDS. American Indians are 1.5 times as likely to have AIDS than Whites.
For Asians and Pacific Islanders, HIV/AIDS is the ninth leading cause of death in men aged 25 to 34. Native Hawaiians/Pacific Islanders are 2.2 times as likely to be diagnosed with HIV infections as the White population.
Quick Facts
African American males have 7.8 times the AIDS rate as White males.
African American women have 20 times the HIV rate as White women.
American Indian/Alaska Native women have almost three times the AIDS rate as non-Hispanic white women.
Hispanic females have 4 times the AIDS rate as non-Hispanic white females.
Native Hawaiian / Pacific Islanders are 2.2 times as likely to be diagnosed with AIDS as the White population.
I find this terribly upsetting. Why does AIDS discriminate?
According to the UN: “Africa has the highest percentage of HIV in 2009 with 15-28%, with Sub-Saharan Africa suffering the most—Ethiopia, Nigeria, South Africa, Zambia, and Zimbabwe. More women than men in Sub-Saharan Africa have HIV. The majority have gotten HIV from unprotected heterosexual sex, often paid sex.”
The statistics show that at the end of 2011, an estimated 230,000 people were living with HIV in the Caribbean. Some 13,000 people were newly infected during 2011, and 10,000 people died from AIDS.1
In the Bahamas more than 3% of the adult population is living with HIV.2 This level of HIV prevalence is found only in sub-Saharan Africa, making the Caribbean the second most affected region in the world.3 Half of adults living with the virus are women.
Overall, the main route of HIV transmission in the Caribbean is heterosexual sex, with many new infections linked with commercial sex work.5 Sex between men is recently emerging as another major route of transmission in Caribbean countries. Cultural and behavioural patterns (such as early initiation of sexual acts, and taboos related to sex and sexuality), gender inequalities, lack of confidentiality, stigmatisation and economic need are some of the factors influencing vulnerability to HIV and AIDS in the Caribbean.
What could be the cultural behavioral patterns that cause high rates of AIDS among blacks? Why do blacks tend to have sex at the youngest ages and orientals tend to wait the longest before having sex?
What about AIDS in Japan? Wikipedia says: “In December 2009, the World Health Organization reports the number of HIV cases in Japan to be at least 17,000.[3] This equates to roughly 0.01% of the population of Japan, one of the lowest ratios of reported HIV in the world.”
When I consult a world map of AIDS rates, I see that AIDS is almost unknown in oriental countries, rare in dominantly white countries, and common in black countries:
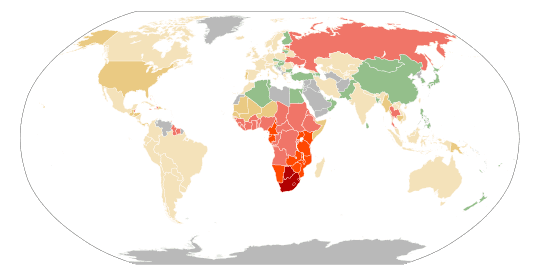
According to Wikipedia: “The table makes clear Africa’s unfortunate position in the worldwide HIV and AIDS epidemic, as the 19 countries worldwide with the highest prevalence of reported infections are all African countries with more than 24.5 million, and more than 60% of the HIV-infected population. South Africa is reported to have the largest population living with the disease, at well over 5 million people infected, followed by Nigeria in 2nd place and India being the 3rd largest population of HIV infected with more than 2 million people reported due to its large overall population, but with a prevalence rate of 0.30 in comparison to the prevalence rate of 0.60 in US and 18.10 in South Africa.”
Perhaps AIDS is an anomaly? When it comes to other sexually-transmitted diseases, perhaps orientals have the most and blacks have the least? No. The statistics show that blacks are far more likely to have STDs and orientals are the least likely.
Surveillance data show higher rates of reported STDs among some racial or ethnic minority groups when compared with rates among whites. Race and ethnicity in the United States are population characteristics that also correlate with other fundamental determinants of health status.1,2
Social and economic conditions, such as high rates of poverty, income inequality, unemployment, low educational attainment and geographic isolation can make it more difficult for individuals to protect their sexual health.3 People who struggle financially are often experiencing life circumstances that increase their risk for STDs.4 Those who cannot afford basic necessities may have trouble accessing and affording quality sexual health services.5 As an example, in 2010, the poverty rates, unemployment rates, and high school drop-out rates for blacks, American Indians/Alaska Natives, and Hispanics were considerably higher than for whites, differences commensurate with observed disparities in STD burden.6–9 Many people of Hispanic ethnicity face additional barriers arising from immigration or undocumented citizenship status.10 Even when health care is available, fear and distrust of health care institutions can negatively affect the health careseeking experience for many racial/ethnic minorities when there is social discrimination, provider bias, or the perception that these may exist.11,12
In communities where STD prevalence is higher, individuals may have a more difficult time reducing their risk for infection. With each sexual encounter, they face a greater chance of encountering an infected partner than those in lower prevalence settings.13 Acknowledging the inequity in STD rates by race or ethnicity is one of the first steps in empowering affected communities to organize and focus on this problem.
Blacks—In 2012, the overall rate among blacks in the United States was 1,229.4 cases per 100,000 population (Table 11B). The rate of chlamydia among black women was over six times the rate among white women (1,613.6 and 260.5 per 100,000 females, respectively) (Table 11B and Figure L). The chlamydia rate among black men was over eight times the rate among white men (809.2 and 95.9 cases per 100,000 males, respectively).
Chlamydia rates were highest for blacks aged 15–19 and 20–24 years in 2012 (Table 11B). The chlamydia rate among black females aged 15–19 years was 7,719.1 cases per 100,000 females, which was over five times the rate among white females in the same age group (1,458.3 per 100,000 females). The rate among black women aged 20–24 years was 4.4 times the rate among white women in the same age group (Table 11B).
Similar racial disparities in reported chlamydia rates exist among men. Among males aged 15–19 years, the rate among blacks was 9.9 times the rate among whites (Table 11B). The chlamydia rate among black men aged 20–24 years was six times the rate among white men of the same age group (3,556.0 and 590.6 cases per 100,000 males, respectively).
Asians— In 2012, the chlamydia rate among Asians was 112.9 cases per 100,000 population (Table 11B). The overall rate among whites is 1.6 times the rate among Asians.
Hispanics— In 2012, the chlamydia rate among Hispanics was 380.3 cases per 100,000 population (Table 11B) which is over two times the rate among whites.
The rate of gonorrhea among blacks in 2012 was 462.0 cases per 100,000 population, which was 14.9 times the rate among whites (31.0 per 100,000) (Table 22B). This disparity has decreased slightly in recent years (Figure M). This disparity was larger for black men (16.2 times) than for black women (13.8 times).
Black men aged 20–24 years had a gonorrhea rate of 1,903.7 cases per 100,000 men, which was 16.4 times the rate among white men in the same age group (115.9 per 100,000). Black men aged 15–19 years had a gonorrhea rate of 1,012.3 cases per 100,000 men, which was 26.2 times the rate among white men in the same age group (38.7 per 100,000).
Asians—In 2012, the gonorrhea rate among Asians was 16.9 cases per 100,000 population, which was lower than (0.5 times) the rate among whites (Table 22B). This difference is larger for Asian women than for Asian men…
Hispanics—In 2012, the gonorrhea rate among Hispanics was 60.4 cases per 100,000 population, which was 1.9 times the rate among whites (Table 22B). This disparity was larger for Hispanic men (2.2 times) than for Hispanic women (1.8 times)…
Syphillis:
Blacks — In 2012, 39.7% of all cases reported to CDC were among blacks. The overall 2012 rate for blacks was 6.1 times the rate for whites. In 2012, the rate of P&S syphilis among black men was 5.7 times the rate among white men; the rate among black women was 16 times the rate among white women…Asians — In 2012, 1.9% of all cases reported to CDC were among Asians. The 2012 rate of P&S syphilis for Asians was 2.0 cases per 100,000 population, which was 0.7 times the rate for whites…
Hispanics— In 2012, 19.5% of all cases reported to CDC were among Hispanics (an increase from 16.7% of all cases in 2011). The 2012 rate of P&S syphilis for Hispanics was 5.7 cases per 100,000 population, which was 2.3 times the rate for whites…
In his book Race, Evolution and Behavior, Philippe Rushton explained:
Race differences exist in sexual behavior. The races differ in how often they like to have sexual intercourse. This affects rates of sexually transmitted diseases. On all the counts, Orientals are the least sexually active, Blacks the most, and Whites are in between. The races also differ in the number of twins and multiple births, in hormone levels, in sexual attitudes, and even in their sexual anatomy.
The races differ in their level of sex hormones. Hormone levels are highest in Blacks and the lowest in Orientals. This may tell us why Black women have premenstrual syndrome (PMS) the most and
Orientals the least.
The races also differ in testosterone level which helps to explain men’s behavior. In one study of college students, testosterone levels were 10 to 20% higher in Blacks than in Whites. For an older sample of U.S. military veterans, Blacks had levels 3% higher than Whites (see the 1992 issue of Steroids). In a study of university students, Black. Americans had 10 to 15% higher levels than White Americans. The Japanese (in Japan) had even lower levels.
Testosterone acts as a “master switch.” It affects things like self-concept, aggression, altruism, crime, and sexuality, not just in men, but in women too. Testosterone also controls things like muscle mass and the deepening of the voice in the teenage years.
Blacks are sexually active at an earlier age than Whites. Whites, in turn, are sexually active earlier than Orientals. Surveys from the World Health Organization show this three-way racial pattern to be true around the world. National surveys from Britain and the United States produce the same findings.
A Los Angeles study found that the age of first sexual activity in high school students was 16.4 years for Orientals, 14.4 years for Blacks, with Whites in the middle. The percentage of students who
were sexually active was 32% for Orientals but 81% for Blacks. Whites again fell between the two other races. A Canadian study found Orientals to be more restrained, even in fantasy and masturbation.
Orientals born in Canada were just as restrained as recent Asian immigrants. Around the world, sexual activity for married couples follows the three-way pattern. A 1951 survey asked people how often they had sex. Pacific Islanders and Native Americans said from 1 to 4 times per week, U.S. Whites answered 2 to 4 times per week, while Africans said they had sex 3 to 10 times per week. Later surveys have confirmed these findings. The average frequency of intercourse per week for married couples in their twenties is 2.5 for the Japanese and Chinese in Asia. It is 4 for American Whites. For American Blacks it is 5.
Racial differences are found in sexual permissiveness, thinking about sex, and even in levels of sex guilt. In one study, three generations of Japanese Americans and Japanese students in Japan had less interest in sex than European students. Yet each generation of Japanese Americans had more sex guilt
than White Americans their age. In another study, British men and women said they had three times as many sexual fantasies as Japanese men and women. Orientals were the most likely to say that sex has a weakening effect. Blacks said they had casual intercourse more and felt less concern about it than whites
did.
Race differences in sexual behavior have results in real life. They affect sexually transmitted disease rates. The World Health Organization takes note of sexual diseases like syphilis, gonorrhea, herpes and chlamydia. They report low levels in China and Japan and high levels in Africa. European countries are in the middle.
The racial pattern of these diseases is also true in the U.S. The 1997 syphilis rate among Blacks was 24 times the White rate. The nationwide syphilis rate for Blacks was 22 cases per 100,000 people. It was 0.5 cases per 100,000 for Whites, and even lower for Orientals. A recent report found up to 25% of inner city girls (mainly Black) have chlamydia.
Racial differences also show in the current AIDS crisis. Over 30 million people around the world are living with HIV or AIDS. Many Blacks in the U.S. do get AIDS through drug use, but more get it
through sex. At the other extreme, more AIDS sufferers in China and Japan are hemophiliacs. European countries have intermediate HIV infection rates, mostly among homosexual men.
Chart 5 shows the yearly estimates of the HIV infection rate in various parts of the world from the United Nations. The epidemic started in Black Africa in the late 1970s. Today 23 million adults there are living with HIV/AIDS. Over fifty percent of these are female. This shows that transmission is mainly heterosexual. Currently, 8 out of every 100 Africans are infected with the AIDS virus and the epidemic is considered out of control. In some areas the AIDS rate reaches 70%. In South Africa one in 10 adults is
living with HIV.
The HIV infection rate is also high in the Black Caribbean. About 2%! Thirty-three percent of the AIDS cases there are women. This high figure among women shows that the spread tends to be from
heterosexual intercourse. The high rate of HIV in the 2,000 mile band of Caribbean countries extends from Bermuda to Guyana, and it seems to be the highest in Haiti, with a rate close to 6%. It is the most infected area outside of Black Africa.
Data published by the U.S. Centers for Disease Control and Prevention show that African Americans have HIV rates similar to the Black Caribbean and parts of Black Africa. Three percent of
Black men and 1% of Black women in the U.S. are living with HIV (Chart 5). The rate for White Americans is less than 0.1%, while the rate for Asian Americans is less than 0.05%. Rates for Europe and the Pacific Rim are also low. Of course AIDS is a serious public health problem for all racial groups, but it is especially so for Africans and people of African descent.
The three-way pattern of race differences is found in rates of multiple births (two-egg twinning), hormone levels, sexual attitudes, sexual anatomy, frequency of intercourse, and sexually transmitted diseases (STDs). Both male and female sex hormone levels are the highest in Blacks, the lowest in Orientals, with Whites in between. Sex hormones affect not only our bodies, but also the way we act and think. Blacks are the most sexually active, have the most multiple births, and have the most permissive attitudes. Orientals are the least sexually active and show the least sexual fantasy and the most sexual guilt. Whites are in the middle. Sex diseases are most common in Blacks, least so in Orientals, with Whites in between the two. The very high rate of AIDS in Africa, the Black Caribbean and in Black Americans is alarming.